


Copenhagen Research Group for Inflammatory Skin (CORGIS), Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, Hellerup, Denmark
The immune mechanisms involved in atopic dermatitis (AD) are complex and little is known about the possible role of the gut microbiota in the aetiopathogenesis of AD. A systematic review of the literature was performed according to PRISMA guidelines, and included 44 of 2,199 studies (26 observational and 18 interventional studies). Detection of gut microbiota was performed by either 16s rRNA PCR, or by culture. Observational studies were diverse regarding the age of study participants and the bacterial species investigated. Overall, the results were conflicting with regard to diversity of the gut microbiota, specific bacterial colonization, and subsequent risk of AD. Nearly half of the included interventional studies showed that an altered gut microbial colonization due to use of probiotics had a positive effect on the severity of AD. The remaining studies did not show an effect of probiotics on the severity of AD despite an alteration in the gut microbial composition. The role of the gut microbiome for the onset and severity of pre-existing AD remains controversial.
Key words: atopic dermatitis; gut; microbiome.
Accepted Jul 27, 2018; Epub ahead of print Aug 7, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Peter Jensen, Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, Kildegårdsvej 28, DK-2900 Hellerup, Denmark. E-mail: peter.jensen@regionh.dk
Atopic dermatitis (AD) a chronic inflammatory skin disease with complex immune mechanisms. Research interest in the role of the intestinal microbiome in the regulation of cell-mediated immune pathways is increasing. We performed a systemic review summarizing studies investigating the role of the gut microbiota in AD.
We included 44 studies, 26 observational, and 18 interventional studies. Overall, the results were conflicting. Nearly half of the included interventional studies showed that an altered gut microbial colonization by use of probiotics had a positive effect on the severity of AD. The role of the gut microbiome in AD remains controversial.
Atopic dermatitis (AD) is a common chronic inflammatory skin disease with a worldwide prevalence of approximately 20% in children and 2–5% in adults (1). In recent years, there has been an increasing interest in the role of the intestinal microbiota in the aetiopathogenesis of AD. The gut microbiota increases in diversity over time, especially during the first 5 years of life, and the gut bacterial composition is unique at the individual level (2). The adult gastrointestinal tract houses several trillion microbial cells. Studies in humans have identified a total of 9.9 million microbial genes in the adult intestine.
The gut microbiota is involved in the regulation of a wide range of physiological processes, such as intestinal endocrine function, cell proliferation, vascularization, biosynthesis of various compounds, and elimination of toxins (2). Cell-mediated immune pathways, and development and maintenance of the gut mucosa are also influenced by the gut microbiota (3). Imbalance or dysbiosis of the human gut microbiota during early childhood may be a risk factor for a wide range of lifestyle-related and immune-mediated diseases, such as asthma, metabolic diseases, and inflammatory bowel disease (4–6). Also, studies examining the effect of an altered gut microbial composition, i.e. through faecal transplantation, have shown promising results in atherosclerosis, intestinal infection, and certain cancers (2). Studies on germ-free mice suggest that the absence of intestinal bacteria may lead to immune dysfunction, which may increase the risk of disease later in life (7–9).
The immune mechanisms in AD are complex and little is known about the role of the gut microbiome in the pathogenesis of AD. The aim of this study was to review the existing literature on the role of the gut microbiota in the aetiopathogenesis and severity of AD.
A systematic review was performed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines (10). Prior to study start, the search string, objectives and study protocol methods were defined.
PubMed was searched (on 13 June 2017) for studies and trials that aimed to investigate the role of the gut microbiota in AD. The following search string was used: ((Atopic Dermatitis OR Atopic Eczema) AND (Intestine OR Microbiota OR Intestinal Microbiome OR Intestinal microflora OR Gastrointestinal microbiome OR Gut microbiome)). Additional studies were identified from the reference lists of already included studies.
Articles in English, which included patients diagnosed with AD and/or healthy controls, were included. The studies were either interventional or observational and had to evaluate the gut microbiota and its association with AD. Studies that did not analyse the faecal microbiota were excluded, as were animal studies, letters to the Editor, case reports, and articles not written in English.
Two authors, EB and PJ, performed the PubMed search and screening of eligible articles. In case of discrepancy or doubt, the articles in question were discussed in the research group and consensus was reached. The studies were separated into observational and interventional studies and the following information was extracted from each article: observational studies: author, design, study population (number of participants and their age), type of exposure, age at faecal sampling, method of bacterial analysis, study outcome, number of study subjects who developed AD, and statistically significant results. Interventional studies: author, design, study population (number of participants, age, and severity of AD), objective, type of and duration of intervention, time points of faecal sampling(s), method of bacterial analysis, alterations of the gut microbiome, severity of AD, time-points at which the severity of AD was measured, and changes in the severity of AD.
Summary of measurements: AD diagnosed with the UK Working Party’s (UKWP) Diagnostic Criteria for Atopic Dermatitis or Hanifin & Rajka Criteria for Atopic Dermatitis (7, 11). Severity of AD assessed was mostly assessed by SCORing AD (SCORAD) (12)
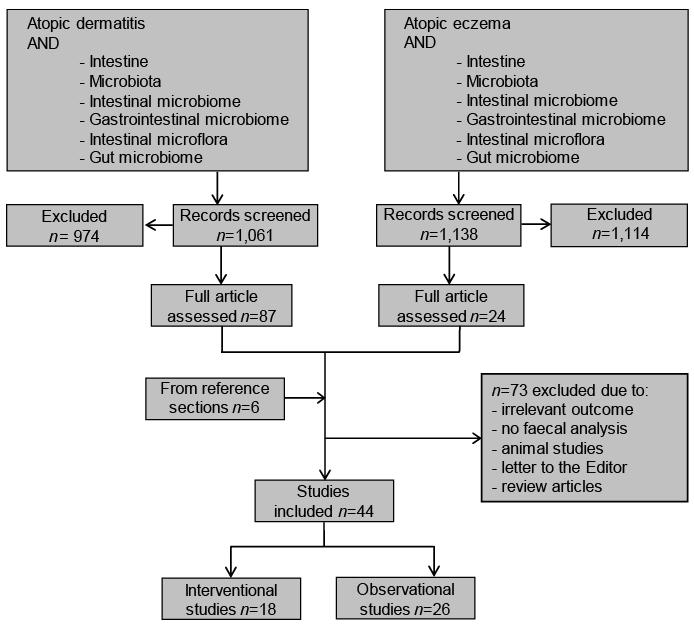
The initial search revealed a total of 2,199 citations. Of these, 2,088 studies were excluded based on title and/or abstract. The remaining 111 studies were screened by full-text read, and, of these, 73 articles were excluded for failing to meet the inclusion criteria, leaving 38 articles. An additional 6 articles were identified from the reference sections of other articles. In total, 44 studies were included in this systematic review, of which 26 were observational and 18 interventional (Fig. 1).
Fig. 1. Research strategy.
The 26 observational studies consisted of 17 prospective cohort studies (13–29) and 9 case-controlled studies (30–38) (Table I).
Table I. Observational studies
The observational studies included a total of 4,257 children. The majority of studies included infants who had at least one parent with either AD or atopy. In most studies, the patients were excluded if they had received antibiotic treatment up to one month prior to inclusion or during the particular study period. The studies used different inclusion criteria, and also, there was variation with regards to mode of delivery (caesarean section/vaginal route), and type of nourishment during infancy (breast milk/weaning patterns/formula diet). Furthermore, there was some variation in the reporting of potential confounders, such as maternal smoking habits, residential area, birth weight, and number of siblings. However, in some of the studies, adjustments for these factors were made (13–17, 21, 24, 26–28, 38). Also, there was considerable variation among the studies with regards to the age of the participants and time-points of faecal sampling. In most studies, faecal sampling was performed in infants below the age of 1 year. The studies focused on a variety of different specific bacterial genera or subspecies, i.e. Clostridium, Bacteroides, Lactobacillus, E. coli, and Staphylococcus aureus (Table I). Given the heterogeneity of studies, a narrative synthesis of the findings was conducted.
Out of the 26 observational studies, 11 investigated the diversity of the gut microbiome in relation to new-onset of AD (13–21, 30, 31) (Table I). Overall, the observational studies were quite heterogenic with regard to study population and bacterial exposure. Five studies found no significant differences in the diversity of gut microbiota in healthy participants compared with patients with AD (13, 14, 21, 30, 31). A Danish study including 346 children examined the gut microbiota in infants, but found no association between gut bacterial composition at age 1 month and 12 months and the subsequent development of AD up to the age of 6 years (13). Five studies with a total of 231 children, found that participants who developed AD had a less diverse gut microbiome compared with participants who did not develop AD (15–19) and one study found that an increased gut microbial diversity was associated with subsequent development of AD (n = 34) (20).
Twenty studies investigated specific bacterial colonization patterns in patients with AD compared with healthy controls (14, 19, 20, 22–38). The studies examined different gut bacterial species, but focused mainly on detection of Bifidobacteria, Clostridia, and Lactobacilli. Subspecies of Bifidobacteria were found in both increased and decreased numbers in children with AD (14, 22, 26, 31–33). One large study (n = 957) (28)+(n = 571) (27) demonstrated that a higher concentration of Clostridia in the gut microbiota was associated with an increased risk of new onset AD. However, other investigators (n = 94) found no association between colonization with Clostridia and subsequent development of AD (22). Furthermore, others (n = 681), showed that intestinal colonization with Lactobacillus paracasei reduced the risk of developing AD (24), while other studies showed no difference or a lower colonization of Lactobacillus subspecies in patients with AD compared with healthy controls (22, 36).
All 18 interventional studies were randomized (39–56), 10 were double-blinded (39, 42, 44, 45, 47, 48, 50, 53, 54, 56), and one study was open-label (41) (Table II). There was a total of 2,802 participants, of whom 2,560 were children (39–49) and 242 adults (50–56). The study populations varied with regard to the baseline severity of eczema (mild-to-severe), age (newborns, children and adults), age at faecal sampling, and duration of follow-up (4–16 weeks). In all but one study, in which mare’s milk was used (50), the participants were given probiotics containing sub-species of Lactobacilli (L. acidofiles, L. paracei, L.salivarius) and/or Bifidobacterium (B. lactis, B. animalis, B. bifidum) as a supplement to their normal diet (Table II). The primary outcomes were the severity of AD assessed by SCORAD or the incidence of new-onset AD. The studies focused on a variety of different bacterial species. In the majority of studies, it was attempted to verify the faecal presence of the particular probiotic strain administered per-orally, while other studies aimed to investigate changes from baseline of pre-existing bacterial species (Table II). Again, given the heterogeneity of studies, a narrative synthesis of the findings was conducted.
Table II. Interventional studies
In 3 studies, the participating newborns were fed probiotic supplements (39–41). Two of 3 studies showed that the incidence of new-onset AD was lower in the newborns who had been given probiotics after 6 and 10 months (40, 41). One study included a particularly large sample of patients (n = 925) and found a concomitant alteration of the gut microbiota with a significantly higher concentration of the interventional strains used (40).
A total of 15 studies, which included both children and adults with AD, aimed to investigate the efficacy of probiotics on the severity of AD compared with placebo (42–56). In 8 studies, oral probiotic supplement was superior to placebo and resulted in a significant reduction in the severity of AD (45–47, 49, 53–56). In 7 studies, the severity of AD remained unchanged subsequent to administration of probiotics (42–44, 48, 50–52). In 6 of 8 studies that reported a reduction in the severity of AD, this was associated with a concomitant alteration in the gut microbiome (45, 47, 49, 53, 54, 56). In 7 studies, there was no effect of probiotics on the severity of AD despite a concomitant alteration of the gut microbiome in 6 of these studies (43, 44, 48, 50–52).
A total of 44 studies describing the effect of the gut microbiota on the onset and severity of AD were identified. Nearly half of the interventional studies showed a positive effect of probiotics on the severity of AD, with a concomitant alteration in the gut microbial composition. The remaining studies showed no effect of probiotics on the severity of AD despite a concomitant change in the gut microbial composition. Data from the observational studies were conflicting with some studies showing that participants who developed AD had a less diverse gut microbiome than healthy individuals, while others found no significant differences. Also, observational studies failed to demonstrate overgrowth or lack of specific bacterial species in patients with AD compared with individuals without AD.
The results of the included studies are conflicting and the role of the gut microbiota in the development and severity of AD remains unclear. The conflicting results may be explained by methodological differences, difficulties with isolation and identification of gut bacterial species, and the complexity of the interactions between the gut microbiota and external factors. Methods for detection of bacteria have evolved through the years and are much more sensitive today compared with just 10 years ago (57). The most widely used method for detection of bacteria is the 16s rRNA PCR-DGGE, which is able to detect bacterial species that comprise >1% of the total gut microbiota (29). The so-called shotgun-sequencing approach, a more precise method, is gaining in popularity and has become more affordable and may help to standardize the methodology of bacterial detection in the future (57). Although speculative, it is possible that fungi and viruses may interact with bacteria in the gut, further adding to the complex interplay between gut commensals and host immunity.
The gut microbial composition is different in various regions of the gastrointestinal tract and, therefore, one may argue that faecal analysis may not be representative of the entire gut microbiota (58) (2). In addition, the gut microbiota changes with age (2). This is relevant when interpreting the results, since there was some variation in the age at faecal sampling in the included studies. In the majority of studies, however, faecal sampling was performed at a maximum age of 6 months. Repeated faecal analyses during follow-up would have given a more complete picture of the alterations in the gut microbiota. However, only half of the observational studies included more than 2 faecal samplings (14, 16, 17, 22, 23, 25, 27, 32, 36, 37). Furthermore, the age variation at faecal sampling could have contributed to the conflicting results of the interventional studies, which aimed to examine the efficacy of probiotics on the severity of AD. Bifidobacterium, Streptococcus, Lactococcus and Lactobacillus are among the most abundant bacterial species in early childhood, while Bacteroidetes and Firmicutes are more abundant in the gut microbiota in adulthood (59). This has to be taken into account when interpreting and comparing the results of interventional studies including different age groups aiming to describe the efficacy of probiotics on the severity of AD. Along those lines, Larsen et al. (48) observed a notable inter-individual variation among the included patients.
One study found that treatment with probiotics led to a reduction in the number of participants who developed AD, with a concomitant change in the gut microbiota (40). This is in line with the hypothesis that early exposure to bacteria may affect the development of the immune system in early childhood (60, 61). Interestingly, this study highlights the question as to whether changes in the gut microbiota may reduce the risk of now-onset AD in high-risk children. It remains to be established if patients who are at low-to-moderate risk of AD will benefit from probiotic treatment.
Little is known about the immunological effects of gut microbiota on the pathogenesis of AD (62, 63). However, it has been proposed that probiotics may lead to an induction of regulatory T cells with suppression of interleukin (IL)-10 and TGF-ß (64, 65). Intraperitoneal administration of a Lactobacillus strain in mice has been shown to increase IL-12 and decrease IgE, and in theory this may be beneficial in anaphylaxis, food allergy, and atopy (60). Other studies have demonstrated that germ-free mice have a reduced number of CD4+ T cells compared with controls (66, 67).
This study has several limitations. First, it only included studies available on PubMed. Secondly, the included studies had been conducted in different geographical regions potentially introducing bias due to differences in dietary and hygienic conditions. Given the heterogeneity of the studies, we did not conduct a meta-analysis, but merely a narrative review. This approach was chosen for the following reasons. First, the studies focused on the presence of different bacterial species. Secondly, the severity of AD varied from mild-to-severe comprising the generalizability of the results. Thirdly, the studies included participants from different age groups.
In conclusion, the role of the gut microbiome in AD remains controversial. There is some evidence from larger studies suggesting that administration of probiotics may decrease the risk of new-onset AD. Due to the complexity of the gut microbiome and evolving new techniques within this area of research, further studies are needed to clarify the role of the gut microbiota in the aetiopathogenesis of AD.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize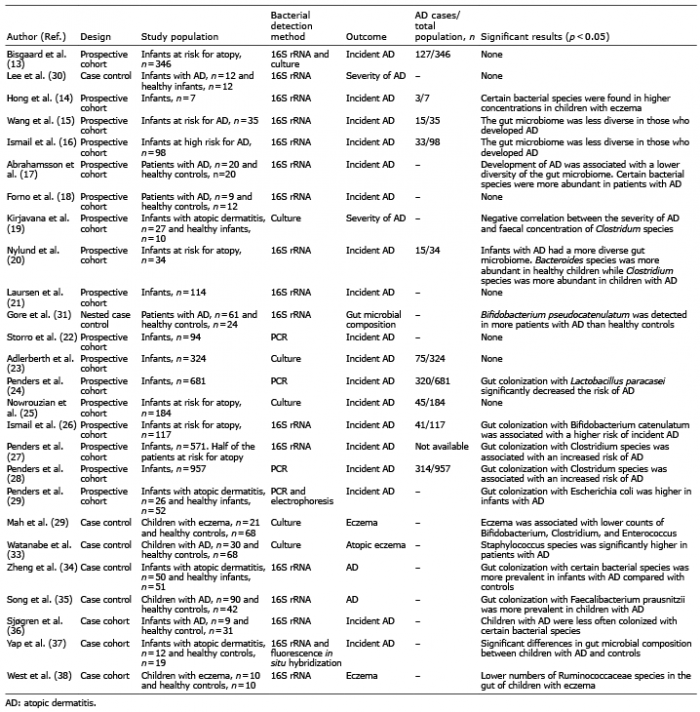 Click to show fullsize
Click to show fullsize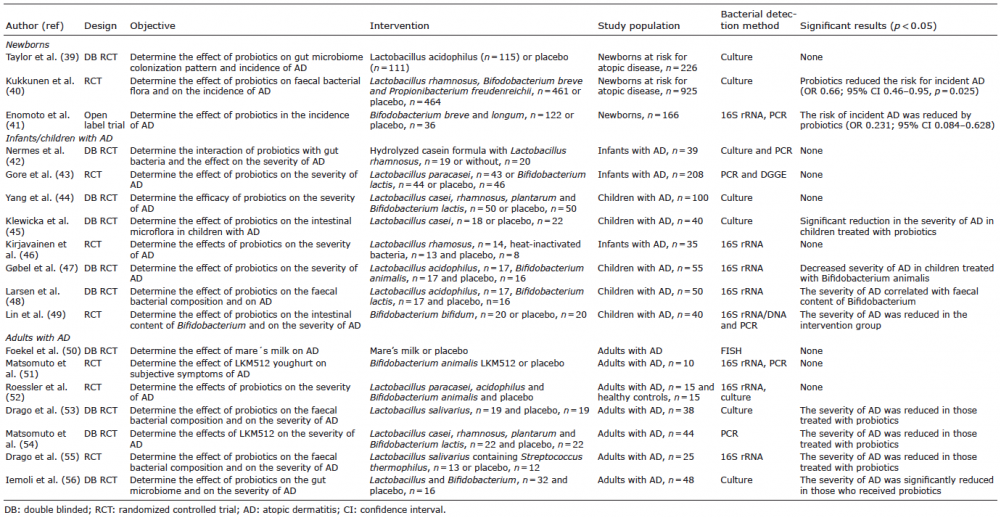 Click to show fullsize
Click to show fullsize